Pharmacological Interventions to Reduce Cognitive Effects of ECT: Review Highlighted by Dr. Andrade in J Clin Psych
Out on PubMed is this commentary by Dr. Andrade:
Reconsideration of the Benefits of Pharmacological Interventions for the Attenuation of the Cognitive Adverse Effects of Electroconvulsive Therapy.J Clin Psychiatry. 2022 Oct 3;83(5):22f14668. doi: 10.4088/JCP.22f14668.PMID: 36198062
The abstract is copied below:
The cognitive adverse effects (AEs) of electroconvulsive therapy (ECT) limit the wider use of the treatment. These AEs can be attenuated by changing the way ECT is administered; however, such changes may reduce the response rate, the speed of response, or both. A recent systematic review and meta-analysis identified more than a dozen pharmacologic interventions in 26 randomized controlled trials (RCTs) that sought to reduce ECT-induced cognitive AEs. Because of large differences across RCTs, only a few outcomes for a few interventions could be pooled in meta-analysis, and most pooled analyses included only 2-3 RCTs. Important findings were that acetylcholinesterase inhibitors, ketamine, memantine, and liothyronine were associated with improved global cognitive functioning at 1-14 days post-ECT. Anti-inflammatory treatments and opioid receptor antagonists were not associated with improvement in general cognitive outcome at 1-14 days post-ECT. Meta-analysis was not possible for the remaining interventions, including piracetam, melatonin, pemoline, nortriptyline, herbal agents, drugs acting on the cortisol pathway, opioid receptor antagonists, l-tryptophan, vasopressin analogs, calcium channel blockers, and others; in individual RCTs, some of these interventions attenuated some cognitive measures as some time points after ECT. Regrettably, none of the RCTs examined clinically meaningful outcomes such as subjective cognitive impairment, impairments in daily life, and persistent autobiographical memory deficits. Future research should study such clinically meaningful outcomes (rather than laboratory tests), using pharmacologic interventions, perhaps in combination, for ECT procedures that are associated with higher cognitive AE burden. A risk is that whatever attenuates ECT-induced cognitive AEs may also attenuate ECT-related therapeutic benefits.
I am very pleased that Dr. Andrade chose our systematic review and meta-analysis to feature in his column in J Clin Psych. His call for additional, targeted research is well taken. Since J Clin Psych is particularly protective of its material, I will just suggest you look it up on their site, and not post anything here.
I have copied below the original blog post about the Verdijk et al. review:
February 09, 2022 Out on PubMed, from investigators in the Netherlands and the USA, in Acta, is this review:
Pharmacological interventions to diminish cognitive side-effects of electroconvulsive therapy: a systematic review and meta-analysis.
Acta Psychiatr Scand. 2022 Jan 24. doi: 10.1111/acps.13397. Online ahead of print.PMID: 35075641 
The abstract is copied below:
Objective: The authors conducted a systematic review and meta-analysis of pharmacological interventions to diminish cognitive side-effects of ECT.
Methods: Electronic databases of Pubmed, PsycInfo, Embase and Scopus were searched from inception through April 1st , 2021 using terms for ECT (e.g., electroconvulsive therapy), cognitive outcome (e.g., cogni*) and pharmacological intervention (e.g., calcium channel blocker, and general terms, like protein). Original studies with humans receiving ECT were included, which applied pharmacological interventions in comparison to placebo or no additive intervention to diminish cognitive side-effects. Data quality was assessed using Risk of Bias and GRADE. Random-effects models were used. PROSPERO registration number was CRD42021212773.
Results: Qualitative synthesis (systematic review) showed 52 studies reporting sixteen pharmacological intervention-types. Quantitative synthesis (meta-analysis) included 26 studies (1387 patients) describing twelve pharmacological intervention-types. Low-quality evidence of efficacy was established for memantine (large effect size) and liothyronine (medium effect size). Very low-quality evidence shows effect of acetylcholine inhibitors, piracetam and melatonin in some cognitive domains. Evidence of no efficacy was revealed for ketamine (very low-quality), herbal preparations with anti-inflammatory properties (very low to low-quality) and opioid receptor agonists (low-quality).
Conclusion: Memantine and liothyronine are promising for further research and future application. Quality of evidence was low due to differences in ECT techniques, study populations and cognitive measurements. These findings provide a guide for rational choices of potential pharmacological intervention research targets to decrease the burden of cognitive side-effects of ECT. Future research should be more uniform in design and attempt to clarify pathophysiological mechanisms of cognitive side-effects of ECT.
Keywords: Cognitive outcome; Electroconvulsive therapy; Meta-analysis; Pharmacological interventions; Systematic review.
The article is here.
And from the text: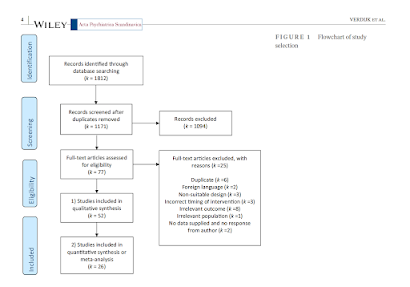



This is an excellent and comprehensive (92 references) systematic review and meta-analysis that I am very pleased to have been a part of. I have always thought that this was an under-researched and very important subject. The thyroid story is particularly intriguing.Kudos to Joey Verdijk for taking the lead in this impressive endeavor, and thanks to the entire Dutch authorship team.I recommend a full read to all ECT practitioners, ~ 25 minutes. (Please see also blog post of Feb. 4, 2022 re Cylert study)
Out on PubMed is this commentary by Dr. Andrade:
Reconsideration of the Benefits of Pharmacological Interventions for the Attenuation of the Cognitive Adverse Effects of Electroconvulsive Therapy.
J Clin Psychiatry. 2022 Oct 3;83(5):22f14668. doi: 10.4088/JCP.22f14668.PMID: 36198062
The abstract is copied below:
The cognitive adverse effects (AEs) of electroconvulsive therapy (ECT) limit the wider use of the treatment. These AEs can be attenuated by changing the way ECT is administered; however, such changes may reduce the response rate, the speed of response, or both. A recent systematic review and meta-analysis identified more than a dozen pharmacologic interventions in 26 randomized controlled trials (RCTs) that sought to reduce ECT-induced cognitive AEs. Because of large differences across RCTs, only a few outcomes for a few interventions could be pooled in meta-analysis, and most pooled analyses included only 2-3 RCTs. Important findings were that acetylcholinesterase inhibitors, ketamine, memantine, and liothyronine were associated with improved global cognitive functioning at 1-14 days post-ECT. Anti-inflammatory treatments and opioid receptor antagonists were not associated with improvement in general cognitive outcome at 1-14 days post-ECT. Meta-analysis was not possible for the remaining interventions, including piracetam, melatonin, pemoline, nortriptyline, herbal agents, drugs acting on the cortisol pathway, opioid receptor antagonists, l-tryptophan, vasopressin analogs, calcium channel blockers, and others; in individual RCTs, some of these interventions attenuated some cognitive measures as some time points after ECT. Regrettably, none of the RCTs examined clinically meaningful outcomes such as subjective cognitive impairment, impairments in daily life, and persistent autobiographical memory deficits. Future research should study such clinically meaningful outcomes (rather than laboratory tests), using pharmacologic interventions, perhaps in combination, for ECT procedures that are associated with higher cognitive AE burden. A risk is that whatever attenuates ECT-induced cognitive AEs may also attenuate ECT-related therapeutic benefits.
I am very pleased that Dr. Andrade chose our systematic review and meta-analysis to feature in his column in J Clin Psych. His call for additional, targeted research is well taken.
Since J Clin Psych is particularly protective of its material, I will just suggest you look it up on their site, and not post anything here.
I have copied below the original blog post about the Verdijk et al. review:
February 09, 2022
Out on PubMed, from investigators in the Netherlands and the USA, in Acta, is this review:
Pharmacological interventions to diminish cognitive side-effects of electroconvulsive therapy: a systematic review and meta-analysis.
Acta Psychiatr Scand. 2022 Jan 24. doi: 10.1111/acps.13397. Online ahead of print.PMID: 35075641
Objective: The authors conducted a systematic review and meta-analysis of pharmacological interventions to diminish cognitive side-effects of ECT.
Methods: Electronic databases of Pubmed, PsycInfo, Embase and Scopus were searched from inception through April 1st , 2021 using terms for ECT (e.g., electroconvulsive therapy), cognitive outcome (e.g., cogni*) and pharmacological intervention (e.g., calcium channel blocker, and general terms, like protein). Original studies with humans receiving ECT were included, which applied pharmacological interventions in comparison to placebo or no additive intervention to diminish cognitive side-effects. Data quality was assessed using Risk of Bias and GRADE. Random-effects models were used. PROSPERO registration number was CRD42021212773.
Results: Qualitative synthesis (systematic review) showed 52 studies reporting sixteen pharmacological intervention-types. Quantitative synthesis (meta-analysis) included 26 studies (1387 patients) describing twelve pharmacological intervention-types. Low-quality evidence of efficacy was established for memantine (large effect size) and liothyronine (medium effect size). Very low-quality evidence shows effect of acetylcholine inhibitors, piracetam and melatonin in some cognitive domains. Evidence of no efficacy was revealed for ketamine (very low-quality), herbal preparations with anti-inflammatory properties (very low to low-quality) and opioid receptor agonists (low-quality).
Conclusion: Memantine and liothyronine are promising for further research and future application. Quality of evidence was low due to differences in ECT techniques, study populations and cognitive measurements. These findings provide a guide for rational choices of potential pharmacological intervention research targets to decrease the burden of cognitive side-effects of ECT. Future research should be more uniform in design and attempt to clarify pathophysiological mechanisms of cognitive side-effects of ECT.
Keywords: Cognitive outcome; Electroconvulsive therapy; Meta-analysis; Pharmacological interventions; Systematic review.
Methods: Electronic databases of Pubmed, PsycInfo, Embase and Scopus were searched from inception through April 1st , 2021 using terms for ECT (e.g., electroconvulsive therapy), cognitive outcome (e.g., cogni*) and pharmacological intervention (e.g., calcium channel blocker, and general terms, like protein). Original studies with humans receiving ECT were included, which applied pharmacological interventions in comparison to placebo or no additive intervention to diminish cognitive side-effects. Data quality was assessed using Risk of Bias and GRADE. Random-effects models were used. PROSPERO registration number was CRD42021212773.
Results: Qualitative synthesis (systematic review) showed 52 studies reporting sixteen pharmacological intervention-types. Quantitative synthesis (meta-analysis) included 26 studies (1387 patients) describing twelve pharmacological intervention-types. Low-quality evidence of efficacy was established for memantine (large effect size) and liothyronine (medium effect size). Very low-quality evidence shows effect of acetylcholine inhibitors, piracetam and melatonin in some cognitive domains. Evidence of no efficacy was revealed for ketamine (very low-quality), herbal preparations with anti-inflammatory properties (very low to low-quality) and opioid receptor agonists (low-quality).
Conclusion: Memantine and liothyronine are promising for further research and future application. Quality of evidence was low due to differences in ECT techniques, study populations and cognitive measurements. These findings provide a guide for rational choices of potential pharmacological intervention research targets to decrease the burden of cognitive side-effects of ECT. Future research should be more uniform in design and attempt to clarify pathophysiological mechanisms of cognitive side-effects of ECT.
Keywords: Cognitive outcome; Electroconvulsive therapy; Meta-analysis; Pharmacological interventions; Systematic review.
The article is here.
This is an excellent and comprehensive (92 references) systematic review and meta-analysis that I am very pleased to have been a part of. I have always thought that this was an under-researched and very important subject.
And from the text:
This is an excellent and comprehensive (92 references) systematic review and meta-analysis that I am very pleased to have been a part of. I have always thought that this was an under-researched and very important subject.
The thyroid story is particularly intriguing.
Kudos to Joey Verdijk for taking the lead in this impressive endeavor, and thanks to the entire Dutch authorship team.
I recommend a full read to all ECT practitioners, ~ 25 minutes. (Please see also blog post of Feb. 4, 2022 re Cylert study)

