ECT in Pregnancy: New Safety and Efficacy Data From Sweden
Out on PubMed, from investigators in Sweden, is this study:
Acta Psychiatr Scand. 2023 Oct 18. doi: 10.1111/acps.13623. Online ahead of print.PMID: 37852926
The abstract is copied below:
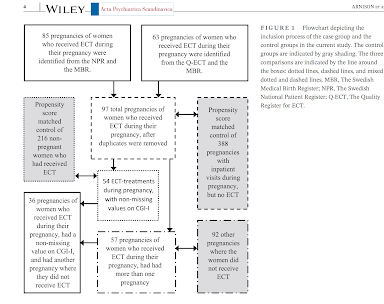
Introduction: Psychiatric disorders are common during pregnancy, affecting up to 16% of pregnant women. Severe depression and anxiety have significant negative effects on the health of both the mother and the developing fetus. Electroconvulsive therapy (ECT) is considered a treatment option for pregnant women with severe psychiatric disorders when other treatments have been ineffective or pose risks to the fetus. Knowledge of the safety and efficacy of ECT during pregnancy, however, remains limited.Methods: Data were obtained from nationwide registries of pregnant women in Sweden who received ECT for a severe psychiatric disorder from January 2008 to December 2021. ECT-related outcomes in pregnant women were compared by propensity score matching with a group of non-pregnant women who also received ECT. Pregnancy-related outcomes were compared with two additional control groups: one consisting of the same group of women who did not receive ECT during another pregnancy and the other composed of pregnant women admitted to inpatient psychiatric care but who did not receive ECT, matched based on propensity score.
Results: Ninety-five pregnant women received ECT during the study period, accounting for 97 pregnancies. The response rate to ECT in pregnant women (n = 54) was similar to the matched control group of non-pregnant women (74% vs. 65%; OR 1.61; 95% CI 0.79-3.27). Rates of adverse events related to ECT were similar to those in the control group. There were no pre-term births or severe adverse outcomes related to the pregnancy, that were close in time to ECT. Therefore, no adverse outcomes related to pregnancy and childbirth could be directly attributed to ECT. The likelihood of premature birth and a 5-min Apgar score <7 in the newborn were both significantly higher in the ECT group, compared with the matched non-ECT group (OR 2.33, 95% CI 1.15-4.73, p = 0.008, and OR 3.68, 95% CI 1.58-8.55, p < 0.001, respectively). By contrast, no significant differences were observed when women in the pregnant ECT group were compared with the same group lacking ECT during another pregnancy.
Conclusions: ECT was associated with a positive treatment response in pregnant women with severe psychiatric disorders. The response rate to ECT was similar in pregnant and non-pregnant women. Nevertheless, the risks of premature birth and of a slightly poorer condition in newborns were higher in women who did than did not receive ECT, emphasizing the need for increased attention to severe psychiatric disorders during pregnancy.
Keywords: electroconvulsive therapy; fetus; newborn; pregnancy; women.
The paper is here.
And from the text:


While we don't know everything about ECT in pregnancy, as these authors correctly state, we certainly know enough to consider ECT a standard treatment option in appropriately selected pregnant patients with severe mood and psychotic disorders.
Kudos to our Swedish colleagues for this authoritative contribution to the ECT literature.


The below comment is from Dr. Max Fink:
ReplyDeleteMonitoring of Pregnant Mothers during ECT
When we began to admit pregnant women for ECT, our OB consultant recommended fetal heart rate monitoring during the seizure. We were surprised that the fetal heart rate did not increase with the increased maternal heart rate during the ECT seizure. A few minutes after the maternal seizure the fetal heart rate increased by 5-10 bpm for a few minutes. After we treated a half dozen cases, the OB consultant agreed to dispense with fetal heart rate monitoring.
All our pregnant women treated with ECT were positioned on the lateral position.
Max Fink, M.D.
Stony Brook University